

Is anxiety catching?
Negative expectations and the social transmission of anxiety

Yes, anxiety is catching. You can stop reading now. (I hope you won’t.)
This week’s Substack is slightly different from previous editions. I have a paper in this month’s British Journal of Psychiatry on ‘Nocebo mechanisms in the social transmission of anxiety’: how the negative placebo effect contributes to the spread of anxiety through friends, acquaintances and wider culture. I’m not going to replicate the paper; you can read it here, if you’re interested. Instead, I’m going to outline some of its themes: evidence that anxiety is socially transmissible, the nocebo effect and how it works, and how the nocebo effect may be involved in how anxiety spreads between people.
First up: anxiety can sometimes be catching. It is clearly not catching in the precise way that a cold is: there is no virus or other organic disease process at play. Instead, it can transmit through social processes – through ideas, language, behaviours and other ways of communicating distress. Even when researchers control for the effects of genetics, data on families of twins show that anxiety can be passed from parents to their children. Friends can share similar levels of anxiety. This is sometimes due to our tendency to seek out people who are similar to ourselves; in other cases, anxiety can be passed on through processes such as co-rumination – endlessly dissecting problems and discussing concerns.
Cultural norms, general knowledge and templates of illness can also contribute to the social transmission of anxiety. This takes place beyond the well-established truth that social and economic factors influence individual mental health (job insecurity during recessions, for example, is unsurprisingly linked to increased anxiety). When we are feeling distressed, our symptoms tend to take shape according to whichever illnesses are made acceptable by current norms. Hysteria was once common. Today, it’s anxiety.
Next up: what is the nocebo effect and how does it affect the spread of symptoms?
Nocebo has sometimes been described as a negative placebo, translated from Latin as ‘I will harm’. The placebo effect occurs when a person takes something inert, such as a sugar pill or a saline injection, and experiences a boost in physical or mental health. This is commonly seen in clinical trials when participants are unaware whether they’re taking an active drug or a placebo, but the placebo effect is visible even when people know they’re taking a placebo. A placebo response describes the treatment boost combined with other positive ‘white coat’ effects – the clinical environment, the expectation of care and concern from clinicians, the subtle cues of therapeutic language.
The nocebo effect (and response) describes the opposite. Expecting harm from something that shouldn’t cause it reliably brings this harm to pass: for example, people experience more pain from an injection when they are told it will hurt. Nocebo effects don’t just bring about subjective symptoms such as low mood, itchiness and nausea. They cause measurable, physical changes: asthma patients have been shown to develop inflamed airways, for example, when told a harmless smell can cause their symptoms to worsen. Expectation of harm causes harm, even beyond nocebo pills, injections or other benign stimuli. In one study, researchers randomly assigned people to receiving information that they were at high or low genetic risk of developing disease. Those in the high-risk category saw a measurable dip in their cardiorespiratory capacity. (Subtext: be careful of genetic profiling.)
Nocebo responses have been implicated in the development of many socially transmissible illnesses, from mass teenage fainting episodes to ‘wind turbine syndrome’ (illness from living near wind farms, thought to arise from belief that wind turbines are causing harm) and even non-coeliac gluten sensitivity. The symptoms they produce are real. According to the authors of The Nocebo Effect: When Words Make You Sick:
‘Even if nocebo effects are caused by negative expectancies, this does not mean that they are merely “all in the head.” Nocebo effects are just as real as regular side effects or symptoms, and people do suffer from them. Because of this, it is important that we find a way to deal with them.’
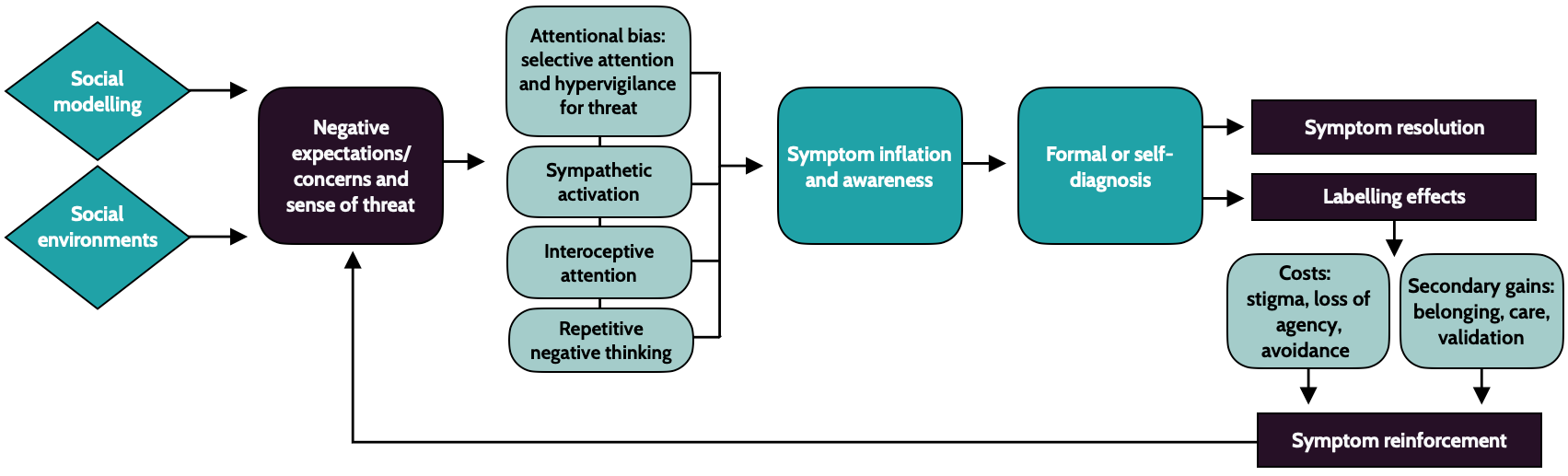
How do nocebo effects and broader responses link to the social transmission of anxiety? We don’t know, for certain, but there’s enough information out there to suggest a process. This is what my piece in The British Journal of Psychiatry attempts to do. The text below describes my model (shown above):
‘Socially informed negative expectations lead to threat-related attentional bias in the form of selective attention (focusing in on potential threats) and hypervigilance (horizon scanning for threats). They also activate the sympathetic nervous system and lower parasympathetic activity. Threat increases interoceptive attention, and may make individuals falsely believe they are experiencing physical anxiety-related symptoms, such as an increased heart-rate. Repetitive negative thinking has been found to mediate the link between negative concerns and anxiety.
‘Symptoms are activated and inflated through these processes. Anxiety is predicted by selective attention to threat, hypervigilance for threat, sympathetic nervous system activation, interoceptive processing and repetitive negative thinking. Once individuals are aware of symptoms, they diagnose themselves or seek formal diagnosis.’
Reinforcement is then key. According to my paper, ‘The resulting labels, such as generalised anxiety disorder, have a variety of negative and positive reinforcement effects. Resulting stigma can lead to more negative self-perception and worse treatment by others; labels can make some individuals believe they lack agency over their condition, further undermining well-being; and having an anxiety diagnosis makes some individuals avoid situations that cause them anxiety, resulting in symptom persistence or progression. Positive reinforcement mechanisms include secondary gains such as a sense of belonging, care and attention from others, and symptom validation. These labelling effects reinforce symptoms, which create further negative expectations or concerns and a sense of threat, creating ongoing feedback loops.’
This is not a proven model. It’s a theory about how nocebo mechanisms contribute to the social transmission of anxiety. We need more studies to know if it’s right, but it does fit reasonably well with existing knowledge.
If it is correct, what does it mean for the real world? One implication is that we need to be careful about how we communicate potential harms – especially to adolescents, who are in the middle of identity formation (identifying as anxious may make the label hard to shake off). For professionals – doctors, therapists and other mental health professionals, teachers and the like – it means being careful not to impart an expectation of fragility among patients, clients and students, as well as knowledge of potential symptom reinforcement mechanisms.
I think the most exciting takeaway is the value of nocebo education. Research shows that nocebo education reduces false self-diagnosis of ADHD, for example; and nocebo education also reduces the likelihood of developing other socially transmitted symptoms, including those that form part of wind turbine syndrome. It seems plausible, at least, that knowledge of nocebo responses could similarly help to reduce the social transmission of anxiety.
The simple act of reading this Substack may have made you more resilient.
Evidence-Based Parenting is available here and Teenagers: The Evidence Base can be found here.
Information about my next book will be available on this Substack later in 2026.
Excellent article Matilda. It reminded me of this TED Talk by Tiffany Watt-Smith on how nostalgia used to be seen as a deadly illness https://youtu.be/S-3qnZrVy9o?si=F5iR5sQxegzUNFNw
Are there examples of social contagion being a positive thing?